Home » Without Label » 30+ awesome pictures Medical Coverage Verification Letter : MDHHS - Premium Assistance Qualifications : This letter is to formally let you know that as of september 30th, 2014, your benefits coverage with cobra will be terminated.
30+ awesome pictures Medical Coverage Verification Letter : MDHHS - Premium Assistance Qualifications : This letter is to formally let you know that as of september 30th, 2014, your benefits coverage with cobra will be terminated.
30+ awesome pictures Medical Coverage Verification Letter : MDHHS - Premium Assistance Qualifications : This letter is to formally let you know that as of september 30th, 2014, your benefits coverage with cobra will be terminated.. Please do not submit this form more than once. A group health plan is any plan of one or more employers to provide health benefits or medical care (directly or otherwise) to current or former employees, the employer, or their families. The portal is fast and easy to use, and online help is available through the eligibility verification process. Please keep this form for your records. If you're in a medicare plan, your plan will send you an evidence of coverage (eoc) each year, usually in the fall.
If you don't have any of these documents, you can submit. A per is done towards the end of the 90 days to verify citizenship. This letter is to formally let you know that as of september 30th, 2014, your benefits coverage with cobra will be terminated. Verification of income and medical insurance coverage this form must be completed by the employer's payroll department.) this form must be hand delivered or mailed to the uf health jacksonville outpatient financial evaluation department at 655 w. Please do not submit this form more than once.
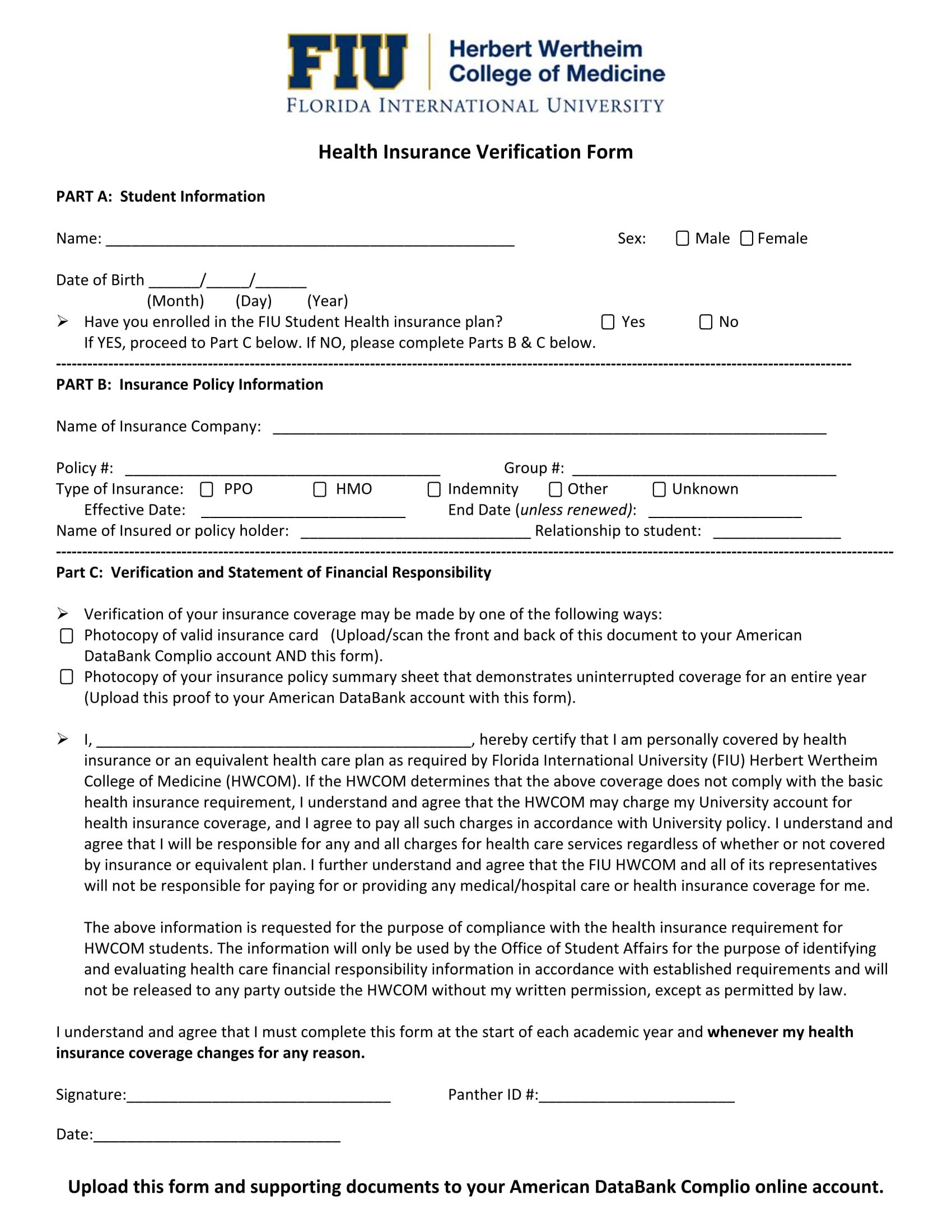
How To Verify Medical Insurance Coverage | Medical ... from www.sequencehealth.com During a per, verification is requested when staff cannot verify the attestation. Please do not submit this form more than once. To understand more about the federal and state individual mandates, please see the information and links below. An example is for a medical insurance verification form which contains the details regarding the health insurance coverage of a member to be used in events of accidents and medical procedures such as surgeries and operations. We only require confirmation that the health plan is an lghp for family members other than the worker or his or her spouse, or for beneficiaries whose. Click on the obtain proof of health coverage button. Verification of ftca coverage for individual providers. Please keep this form for your records.
A letter from an insurance company, on official letterhead or stationery, including:
Use the va blue button tool to view, print, and. Verification of income and medical insurance coverage this form must be completed by the employer's payroll department.) this form must be hand delivered or mailed to the uf health jacksonville outpatient financial evaluation department at 655 w. This letter is to formally let you know that as of september 30th, 2014, your benefits coverage with cobra will be terminated. A per is done towards the end of the 90 days to verify citizenship. An information request letter is mailed to the client. Please do not submit this form more than once. If yes, give the date the coverage began. A group health plan is any plan of one or more employers to provide health benefits or medical care (directly or otherwise) to current or former employees, the employer, or their families. If you don't have any of these documents, you can submit. Health centers are provided their notice of deeming action (nda), together with documentation confirming a covered individual's employment or. 1) letter from employer on their letterhead verifying current coverage; Verify, review, and print documents from your official military personnel file, including your dd 214. Tell us about your recent health coverage, including that you're not.
2) insurance card with your name, the employer's name, and effective date of coverage; If facility or managed care company is not listed on this form you should include the name of the facility, correct mailing address, and to whom the letter should be sent). Use the va blue button tool to view, print, and. A letter or premium bill from your former insurance company that shows you or your dependent's cancellation/termination from health coverage. Learn about the notice of creditable coverage, which your employer or union plan sends you to tell you about medicare savings programs (msps) and the extra help available for medicare prescription drug coverage.
What Is an Insurance Verification Form? [ Uses, Impotance ... from images.sampleforms.com Or click on correspondence/documentation and choose proof of coverage. your coverage letter will be generated and available for download. Health centers are provided their notice of deeming action (nda), together with documentation confirming a covered individual's employment or. Coverage is approved and the client is given 90 days to provide verification of citizenship. When should i get it? If you don't have any of these documents, you can submit. If yes, give the date the coverage began. An example is for a medical insurance verification form which contains the details regarding the health insurance coverage of a member to be used in events of accidents and medical procedures such as surgeries and operations. A per is done towards the end of the 90 days to verify citizenship.
As such, you nor any of your dependents will be eligible for dental, health and vision plans under the company's health plan.
Please do not submit this form more than once. The same requirements, in hi 00805.295c, apply to the disabled beneficiary covered under an lghp, except that the evidence must show that the beneficiary currently has or had coverage under an lghp based on current employment status. For renewals for customers who have selected $250,000 with exclusions, $50,000 in pip medical coverage, or the pip medical opt out (options 4, 5, or 6), a completed and signed pip medical coverage selection form and proof of enrollment in medicaid, medicare, or qualified health coverage must be collected at every renewal. Verification of income and medical insurance coverage this form must be completed by the employer's payroll department.) this form must be hand delivered or mailed to the uf health jacksonville outpatient financial evaluation department at 655 w. When should i get it? During a per, verification is requested when staff cannot verify the attestation. If facility or managed care company is not listed on this form you should include the name of the facility, correct mailing address, and to whom the letter should be sent). A letter or premium bill from your former insurance company that shows you or your dependent's cancellation/termination from health coverage. A decertification letter from your insurance company stating when coverage will no longer be offered. Use this form to request a letter verifying your insurance coverage through mit. 3) printout from insurance website showing your name as a covered dependent , the employer's name, and the effective date of coverage. Please keep this form for your records. Or click on correspondence/documentation and choose proof of coverage. your coverage letter will be generated and available for download.
To receive some benefits, veterans need a letter proving their status. Verification of income and medical insurance coverage this form must be completed by the employer's payroll department.) this form must be hand delivered or mailed to the uf health jacksonville outpatient financial evaluation department at 655 w. Use this form to request a letter verifying your insurance coverage through mit. A letter or premium bill from your former insurance company that shows you or your dependent's cancellation/termination from health coverage. The supporting document must indicate your name, the names of any dependents that were covered under the prior plan and the date the previous health coverage ended.
Medical | Lanny Daise Letters of Recommendation from lannydaise.com To understand more about the federal and state individual mandates, please see the information and links below. If you don't have any of these documents, you can submit. An example is for a medical insurance verification form which contains the details regarding the health insurance coverage of a member to be used in events of accidents and medical procedures such as surgeries and operations. For renewals for customers who have selected $250,000 with exclusions, $50,000 in pip medical coverage, or the pip medical opt out (options 4, 5, or 6), a completed and signed pip medical coverage selection form and proof of enrollment in medicaid, medicare, or qualified health coverage must be collected at every renewal. Click on the obtain proof of health coverage button. A letter from an insurance company, on official letterhead or stationery, including:a letter or premium bill from your former insurance company that shows you or your dependent's cancellation/termination from health coverage.a decertification letter from your insurance company stating when coverage will no longer be offered. Verify, review, and print documents from your official military personnel file, including your dd 214. A letter or premium bill from your former insurance company that shows you or your dependent's cancellation/termination from health coverage.
Click on the obtain proof of health coverage button.
If you don't have any of these documents, you can submit. I request that your office send a letter verifying my medical malpractice coverage to each facility noted on this form (note: 1) letter from employer on their letterhead verifying current coverage; A letter from an insurance company, on official letterhead or stationery, including: A per is done towards the end of the 90 days to verify citizenship. Or click on correspondence/documentation and choose proof of coverage. your coverage letter will be generated and available for download. Letter of explanation to confirm application information if you provide information on your marketplace application that doesn't match our records, you'll need to submit documents to confirm your information. A letter or premium bill from your former insurance company that shows you or your dependent's cancellation/termination from health coverage. Coverage is approved and the client is given 90 days to provide verification of citizenship. 3) printout from insurance website showing your name as a covered dependent , the employer's name, and the effective date of coverage. We only require confirmation that the health plan is an lghp for family members other than the worker or his or her spouse, or for beneficiaries whose. Please do not submit this form more than once. Please complete the required information below.